
El Chapo in Our Backyard
The large print giveth and the small print take the away: on the difference between a drug and a medicine.

I thought that this news story popping up again about Matthew’s Perry’s death was noteworthy.
For those of us not up to date with the details, basically, U.S district attorney of announced that five individuals, including Matthew Perry’s personal assistant and two doctors, have been charged in connection with the actor’s death. The investigation found that the doctors supplied Perry with a large amount of ketamine, taking advantage of his addiction issues to enrich themselves.
So I thought this was deserving a post, not because of his cause of death but because it paints on the hypocritical world we live in, the double standards and the corruption of the spirit of humanity. It also strengthens my exclamation that Covid has caused amnesia in humanity. I mean, isn’t that ironic?! Only four years ago world governments basically bribed doctors to administer drugs, and done it legally!
I have oftentimes declared that our dense dense Maia, has led us to an unprecedented reality in which we are ignorant in spite of knowledge. We have become so intellectually sophisticated to the point in which we have completely forgotten the basic, elementary and simple foundation of things. This robs people - even intelligent people - of their own self reliance.
And so I thought, why not take this case and use it as an opportunity to go back to basics and revisit the concept of drugs and medications (I believe English is the only language in which these two words are used synonymously to describe medicine). Perhaps this double entendre can shine a light to the source of our hypocritical predicament.
The mechanics of medicine
Hippocrates—the same Greek guy after whom the doctors' oath was established, which seems to have become lip service over the years—said:
"The difference between medicine and poison is the dose."
Behind everything is a formula: Any phenomenon; any object; everything living and inanimate is built on patterns. The patterns can be expressed by a formula. When we eat a salad, it is expressed in our body as a formula: A plant is a formula, meat is a formula, bread is a formula, falafel is a formula, and so on and so forth.
Plants are the only species that have no locomotive mechanism: Since they can't move, they can't run away from threats. To deal with this disadvantage, plants have developed the ability to synthesize chemical processes within themselves as a response to these threats.
For instance, when a group of elephants begins feeding on a tree, they don't just consume the leaves—they tear off branches as well, causing significant damage to the tree. When this occurs, the tree sends a warning through the underground root system to the other nearby trees. This triggers a chemical reaction in the surrounding trees, making their leaves bitter or more toxic.
As a result, you'll often notice elephants feeding in one area until the leaves become bitter. At that point, they move on to a distant location to find fresh, unaffected foliage where the warning hasn't yet spread.
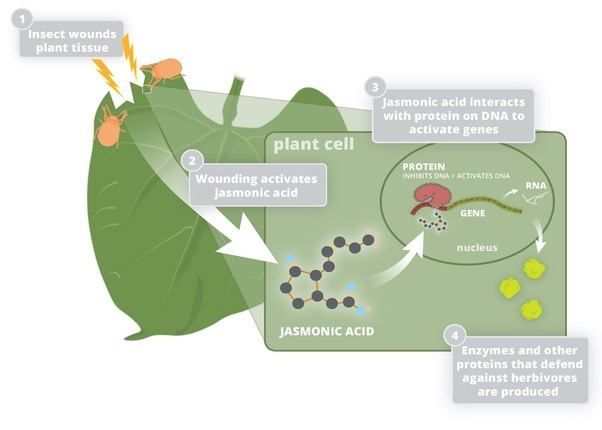
Until the emergence and development of molecular biology, therefore, the science of medicine was the combination and decoction of plants matter, or filtering the material from them in order to use those chemical compounds, in the right dosage, as medicine.
Furthermore, the belief that medicine affects the body is erroneous; in reality, it is quite the opposite. It is the body that acts upon the medicine, not the medicine upon the body. While this assertion may seem unusual, it is nonetheless true.
There is a regulatory agency within the body that maintains its health, known as the "Vital Force." This Vital Force continuously works, day and night, to preserve the body’s health. The moment a harmful or unwholesome substance enters the body, the Vital Force activates, focusing on the task of ejecting the intrusive substance.
For instance, if a particle of dust gets into the eye, there is an immediate and copious flow of tears aimed at flushing the particle out. In many oriental countries, there are various remedial powders called "surma" on the market, which are believed to be beneficial for the eyes by allegedly removing 'heat' from them. When such a powder is applied to the eyes, it immediately causes a profuse flow of tears. The user assumes that the 'heat' has been expelled from the eyes.
In reality, no 'heat' is expelled, nor is any soothing coolness introduced. Instead, nature is simply trying to wash the powder away to protect the eyes from the harmful effects of the poisonous chemical (antimony) in the powder. It is not the 'surma' powder that acts on the eye, but rather the eye that acts on the powder.
The same principle applies to various purgatives, from herbal preparations to milk of magnesia, which are consumed to relieve constipation. The Vital Force strives to expel them as quickly as possible to prevent them from harming the body. And in their expulsion comes the cumulative result felt as the relief of constipation.
Therefore, what we understand from these definitions is that plants produce chemical compounds that, in certain doses, prompt the body to create specific reactions that help mobilize the body's systems and vital force. In turn, these reactions either correct or lead to a state of well-being. Based on Hippocrates' definition, the toxins that plants produce, in the right dosage, have served humanity for centuries as medicines.
And yet, regular use of purgative medicines quickly reveals that the medicine no longer has the desired effect unless the dosage is increased. We then say that the body has become accustomed to or has developed a tolerance to the medication.
If the mechanism was true that the medicine acts on the body, how is it that a medicine that caused a certain effect, when taken in a regular dose, fails to produce the same effect after a period of continuous use, even in larger doses?
The advent of molecular chemistry
With the development of molecular chemistry we developed tools to go deeper into the microscopic world in order to yield a formula that stands behind the observed mechanism. We started experimenting with the formulas behind those "poisons" that those plants created, and from there we took it to the lab. We started duplicating the formulas and synthesizing them synthetically.
Over time, governments established a drug regulatory process to determine toxicity. These regulations require 10 to 12 years of research, at an average cost of about 300 million dollars per medication. After research is approved, the pharmaceutical company owns the patent rights and prices are set to cover this expense.
Today, if common plants need to be approved as medicines, they too are subject to this long and expensive approval process. However, patents cannot be granted on plants or other natural compounds. Therefore, no private enterprise can justify the cost.
Due to this regulatory model, inadvertently, a negative incentive has been formed in which the main premise has become about altering the synthesizing plant formula and patent it in order to recoup the huge investment.
The beginning of the revolving door
If I could draw a line where things begin to become a double-edge sword, it goes back to the implementation of the Bayh-Dole Act of 1980, which has allowed the beneficiaries of federal grants to file patents on work derived from federally funded research. The idea was that the economy would benefit by allowing scientists to be entrepreneurs first, rather than simply publishing their research.
This legislation, however, has undermined health care by bringing the Food and Drug Administration (FDA), and the Centers for Disease Control and Prevention (CDC) into an unholy trinity that serves and promotes private pharmaceutical concerns. So, what we have now is an insidious funding loop. Corporations and pharma lobby to get people elected. Once they're elected, the lobbyists flow an enormous amount of money into the various NIH programs. In the case of NIAID (National Institute of Allergies and Infection Diseases), since 1984, $191 billion have gone through the agency.
As a matter of fact allergies and infectious diseases have increased over 60 fold since that time. Yet somehow a failed agency has gotten $191 billion to solve a problem that is getting worse every single year. The problem is, it's not a company. It’s a money laundering agency. It moves public funds through the hands of a federal agency into the research laboratories, which ultimately are going to conduct research that is then licensed back to the benefactors, which are the pharmaceutical companies that paid to get people into office in the first place.
So, this is a revolving door problem, and the Bayh-Dole Act created an insidious incentive that said that the only research that was going to be conducted was going to be research that ultimately would flow back to the pharmaceutical industry and create juggernauts, where the risk of R&D was taken by the public and the benefit for that R&D was taken by the private sector.

OxyContin
One great example of such procession is the opioid crisis.
Much of this can be attributed to the Sackler family, owners of the now defunct Purdue Pharma, which profited billions from selling OxyContin, a powerful opioid painkiller stronger than morphine, with effects similar to those of heroin.
OxyContin, released in 1996 and was marketed massively as a revolutionary intervention in pain management. Studies show that opioid prescription patterns from 1999 to 2008 were directly linked to the increase in overdose deaths. However, the company knowingly downplayed the drug’s addictive potential.
When request after request was denied, in 1987 the FDA inspector at the time, Dr. Curtis Wright, who initially rejected Purdue’s applications to approve the drug, suddenly approved it for patients with moderate to severe chronic pain. He did so after intense lobbying and courting by the company, which included gifts and an invitation to a three-day hotel conference. Interestingly, after the belated approval of OxyContin, Wright left the FDA and two years later went to work for Purdue Pharma as a consultant with a first-year compensation package of $400,000.
Similarly, U.S. Attorney for the District of Maine, Jay McCloskey, appeared on television in February 2000, announcing that he had sent a letter to all doctors in the state of Maine warning them of the increasing abuse of OxyContin and other opioid-based prescription drugs and the problems therein. However, McCloskey retired from his position in 2001 and subsequently served as a paid consultant for Purdue until 2004. McCloskey also testified for the defense in the Sackler’s' 2007 trial.
Purdue Pharma charged insurance companies for OxyContin by the milligram, meaning the higher the prescribed dosage, the more money the company made. This meant that doctors with high rates of high-dose prescriptions were particularly nurtured by sales representatives.
Purdue Pharma, along with other companies in the painkiller sector, spent nearly $900 million on lobbying and political contributions between 2001 and 2015—eight times more than the gun lobby spent during the same period. Because the drug was approved by the FDA, the company could not be sued as it did not break any laws.
It was only after immense pressure, due to the fact that thousands of people had died from addiction to the drug, that a court ruled the owners of Purdue Pharma, the Sackler family, would be protected from civil lawsuits related to the opioid crisis in exchange for a $6 billion settlement. To this day, many families have yet to see any compensation funds. Since 1999, two hundred thousand Americans have died from overdoses related to OxyContin and other prescription opioids. Needless to say, the family was never prosecuted for liability in criminal court.
Before OxyContin, doctors were very cautious about prescribing opioid-based painkillers, limiting them primarily to cancer patients and end-of-life care. However, Purdue Pharma assured that opioids provided effective pain relief with no risk of addiction, as long as patients took the medication only twice a day.
The gradual release of the drug over time supposedly meant, as sales representatives were told, that pain relief would last 12 hours (in reality, it wore off much sooner, leaving patients with the choice of either taking more pills than prescribed or suffer).
The high price of OxyContin was based on this 12-hour duration, which gave it an advantage over cheaper painkillers that required more frequent dosing. In 2019, former sales representatives came forward and revealed that they were instructed to downplay the risks of addiction during sales pitches, dismissing withdrawal symptoms as a term coined by Purdue called "pseudo-addiction."

Remdesivir’s saga
That didn’t stop with OxyContin. Covid has exposed how egregious and insidious such funding loop is.
The National Institute of Allergy and Infectious Diseases (NIAID) and the Centers for Disease Control and Prevention (CDC) spent $79 million developing Remdesivir for Gilead, which itself distributed $2.45 million during the first quarter of 2020 to promote the drug's use in COVID-19 patients.
During the first eight months of the COVID-19 pandemic, from March to October 2020, the head of the NIAID, Anthony Fauci, issued a directive to all hospitals in the United States to use only one treatment for COVID-19 patients: a drug called Remdesivir.
At that time, Remdesivir was not widely recognized by the medical community. In fact, the FDA website at the time revealed that Remdesivir had never been approved as safe or effective for any disease.
Alongside Fauci's directive stating that "Every doctor in the country should only use Remdesivir," the CDC website in March 2020 referenced two studies designed to prove Remdesivir's efficacy.
The first study was an Ebola trial from 2018 that tested four experimental drugs, including Remdesivir. The second study, sponsored by Gilead (the manufacturer of Remdesivir), involved 53 COVID-19 patients from Japan, Canada, and the United States, who were given Remdesivir for 28 days.
It compared Remdesivir to three other experimental drugs, including one introduced by Fauci, Remdesivir was found to have the highest mortality rate. As a result, the study's safety board withdrew Remdesivir from the trial after six months, deeming it too dangerous to continue. Fauci's experimental drug was also pulled due to its high mortality rate.
The second study, conducted by Gilead and cited by Fauci, reported its findings within 28 days of administering Remdesivir to the 53 COVID-19 patients. The study found that 22% of these patients experienced severe side effects, including multiple organ failure, acute kidney failure, septic shock, and hypertension. Additionally, 8% of the patients had to discontinue the drug by the fifth or tenth day due to its lethal effects. In total, 30% of the patients experienced life-threatening side effects.
Since Remdesivir was the only approved protocol, doctors began administering it via infusion, leading to complications. Patients developed kidney failure (as a result of the drug), which prevented their bodies from excreting fluids, causing pulmonary edema as the fluids accumulated in the chest cavity. This process, in essence, "drowned" the lungs as the kidneys shut down, leading to death by fluid accumulation. This treatment protocol likely contributed to the kidney failure observed in COVID-19 patients during the early months of the pandemic.
On May 1, 2020, the FDA approved Remdesivir for emergency use in hospitalized patients with severe COVID-19, and NIH expert panel members (many with financial ties to Gilead) added the drug to the agency's treatment guidelines. However, the World Health Organization (WHO) recommended against the use of Remdesivir, stating that the drug "does not have a significant effect on mortality or other important outcomes for patients."

I have often said that over the years, academic institutions have been cutting corners and accelerating the training of doctors to speed up their placement in medical institutions. This rush had led to a chain effect, ultimately impacting the patients. The result is of negligence, making medical errors the third leading cause of death in the United States. Each year, approximately 250,000 people die from medical malpractice, a statistic that is at least 20 years old. Since the COVID-19 pandemic, I believe this number has likely risen to over 300,000.
Therefore, during the early months of the COVID-19 pandemic, many doctors mistakenly confused pneumonia with pulmonary edema—two entirely different conditions. They treated patients whose conditions worsened due to the treatment itself, believing the virus was the cause of kidney failure.
Doctors at these hospitals would look at chest X-rays and assume it was secondary pneumonia when, in reality, it was pulmonary edema. There is a clear need for better training to help doctors accurately differentiate between pneumonia and water in the lungs on an X-ray.
On January 21, 2021, the FDA expanded the use of Remdesivir to include "high-risk" adult outpatients and children (12 years of age and older) for the treatment of moderate to severe COVID-19, allowing the drug to be administered intravenously in various outpatient facilities. The FDA's side effect warnings for Remdesivir include potential liver damage and allergic reactions such as "changes in blood pressure and heart rate, low blood oxygen levels, fever, shortness of breath, wheezing, swelling..., rash, nausea, sweating, or shivering."
Such treatments have significantly contributed to the "shockingly high" COVID-19 death rate in the United States compared to the rest of the world, since the U.S was the only country enforcing that one protocol exclusively for the first eight months.
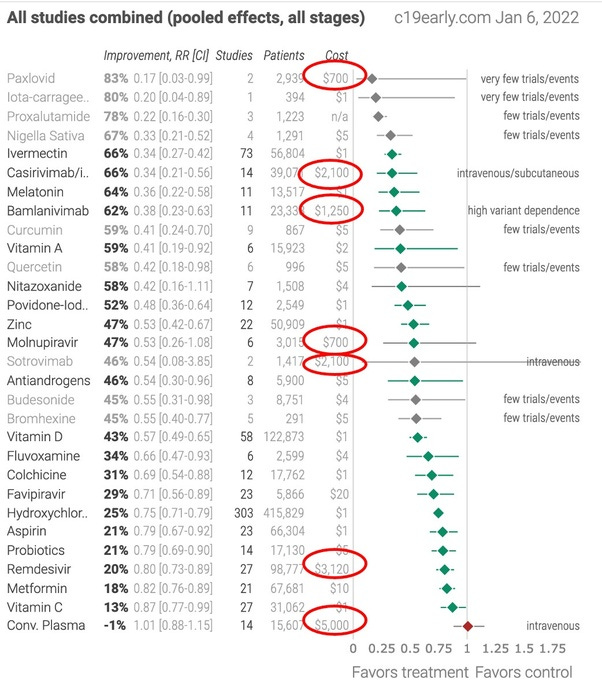
There were dozens of treatments for COVID-19 with multiple peer-reviewed studies proving their effectiveness (such as Hydroxychloroquine (HCQ), Fluvoxamine, and Ivermectin repurposed to treat COVID-19), but they were rejected by a panel of "experts."
The Fareed-Tyson early treatment protocol has been available since March 2020 and has a 99.8% success rate in reducing mortality. The protocol was reported to the NIH in July 2020. Since then, there have been around 850,000 COVID-19 deaths. Had the NIH recommended the Fareed-Tyson protocol when it became known to them, the vast majority of these unnecessary deaths could have been prevented.
It's commonly believed that evidence-based medicine means "the best evidence" dictates the standard of care. In reality, it usually means that financial interests dictate the standard of care, and "evidence" is merely used as a smokescreen to justify profits. The table below provides clear and unequivocal proof of this claim.
The cobra effect
This inadvertently has created the Cobra Effect, which according to Wikipedia is defined as:
"An incentive with an unintended and undesirable result, contrary to the intentions of its designers. When incentives intended to solve a problem instead reward people for worsening it."
The term originated during British colonial rule in India. The British government wanted to address the alarming number of venomous cobras in Delhi. Their strategy was to offer a bounty for each dead cobra. Initially, it was a successful strategy; a large number of cobras were killed for the bounty. However, eventually, enterprising individuals began breeding cobras for income.
When the government realized this, they canceled the bounty program, and the cobra breeders released the now "worthless" snakes, causing the cobra population to increase even more.

The federal government, managed by the U.S. Department of Health and Human Services (HHS), allocated a total of $186.5 billion to the Provider Relief Fund (PRF), with two-thirds of it ($121.3 billion) disbursed as of January 2022. The first tranche of $50 billion went to hospitals and other healthcare providers for healthcare-related expenses or lost revenues starting in April 2020.
In March 2020 the CDC sent documents to every hospital and medical facility in the U.S., providing them with new guidelines on how to diagnose COVID-19.
They explicitly wrote:
"If you find in your clinics or hospitals a patient presenting with flu-like symptoms and they test positive for Influenza A or B, but negative for pneumonia, and you conduct a PCR test that comes back negative for COVID, you can ask the patient where they live, and if the city they live in has positive COVID-19 cases, you can record that person as a positive COVID-19 case, and we will pay you 20% more for every COVID patient compared to a flu patient."
This clause was part of a federal legislation known as the Coronavirus Aid, Relief, and Economic Security Act, or the CARES Act, which included provisions allowing the government to pay more to hospitals specifically for the COVID-19 pandemic. They emphasized the numerous CMS add-ons and other incentives established with the relief act, as well as the 'Paycheck Protection Program and Healthcare Enhancement Act' (PPPHCEA) - highlighting that “payments are contingent upon hospitals' willingness to follow NIH guidelines "for all things related to COVID-19."
The rationale is that this provides a kind of rough "justice" to ensure that hospitals receiving many COVID patients also receive additional funds from the government.
Hospitals complying with these guidelines received grant payments for:
Every diagnostic test completed (required in the emergency room or upon admission).
Every COVID-19 diagnosis.
Every COVID-19 admission.
Use of Gilead's intravenous drug Remdesivir (brand name Veklury), which yields a 20% bonus payment on every hospital bill.
Mechanical ventilation.
'COVID-19' listed as the cause of death.
Payments ranged from $166,000 per COVID patient in Tennessee hospitals, for example, to much higher payments in states like North Dakota ($339,000), Nebraska ($379,000), and West Virginia ($471,000). Additionally, for hospitals found in "COVID-19 hotspots," the HHS distributed funds such as $77,000 per hospitalization initially, followed by $50,000 per hospitalization.

It is crucial to remember that the diagnosis of COVID-19 is based on the Dorsten test (PCR) specifically designed to determine whether a person has COVID-19 or not. However, the test is not sufficiently differential because one thing to remember is that the flu "mysteriously" disappeared in 2020. There were 0 cases of the flu.
The PCR test often returns negative results even during active infection. Additionally, false positives, false negatives, cross-reactivity, and other phenomena - all are common in such tests. Viruses constantly change their genetic structure and mutate in ways that make them invisible to the test.
A significant portion of patients were hospitalized for something unrelated to COVID-19 but were "converted" to COVID patients due to mandatory testing with every admission. And if you consider that PCR tests are highly inaccurate, we begin to see the domino effect of the Cobra Effect.
According to researchers who examined hundreds of hospital admission charts, 40 to 45 percent of the admissions they reviewed were for other reasons, such as cancer treatment or a psychiatric episode, and the COVID diagnosis was incidental. In other words, about a third to half of all hospitalized patients appearing on pandemic data dashboards for COVID-19 in 2021 may have been admitted for a completely different reason or only had a mild presentation of illness.
From that point onward, any patient who died but was diagnosed with COVID-19 through a sequence test, even if they were hospitalized for something unrelated to COVID-19, were recorded as "deceased from COVID-19” so the hospitals can cash in on the reward.
Conclusion:
We began by defining what constitutes a drug and distinguishing it from a medication. However, by this essay, it becomes clear that there is no real difference between the two.
Drugs and medications are essentially the same thing. Both are based on chemical formulas. The term "drug" / “narcotic” is a societal invention, used to draw a line between regulated chemical formulas and those made illicitly or unregulated, like in the black market.
From the body's perspective, however, there is no distinction. The body does not understand the labels and definitions imposed by our intellect; it simply processes the chemical formula that induces reactions within it. In the case of illicit drugs we’re conditioned to fear them because they create dependence and addiction and they lead to associated social problems. But isn’t it the same with regulatory “drugs'' - i.e. medications?!
Since the pharmaceutical industry no longer prioritize the well-being of patients, but rather its primary goal is to generate profit, the same logic that governs drug cartels applies to the pharmaceutical complex of modern medical science. The main premise is the accumulation of wealth at the expense of the "customers'" dependency on the product over time.
This brings us to the current reality where medical science has been "hijacked" by taking the Hippocratic model of medicine—which posits that the patient's well-being is the core essence—and commercializing it into a cartel.
This distorted model places patient well-being in direct opposition to investors' yearnings. The more people remain sick, or the less their illnesses are truly resolved, the more they continue to "purchase" pharmaceutical products and healthcare services.
Media outlets continue to report on drug dens being discovered, or notorious criminals like El Chapo being apprehended, and how vital it is for the safety of our communities, but in reality, the pharmaceutical cartel dwarfs them all. It has become an enormous octopus, extending its tentacles into every sector, be it governmental, corporate, or private. It is everywhere.
The CDC is not an independent agency; it is a vaccine company. The CDC holds over 20 patents on vaccines and sells about $4.6 billion worth of vaccines annually. Several federal investigations, including ones by Congress and the U.S. Senate, as well as the HHS Office of the Inspector General, paint the CDC as a cesspool of corruption, mismanagement, and dysfunction, with alarming conflicts of interest tainting its research, regulatory, and policy-making roles.
Despite the existence of several successful and effective healing systems in this country, the medical system is the only one that receives unwavering government support. All health departments, hospitals, and institutions supported by taxpayers' money are under the control of the pharmaceutical establishment.

Modern drug couriers
Remarkably, like any good and efficient cartel, its footprint must be substantiated by an army of foot soldiers: the drug dealers on the street. And so, doctors nowadays have become the foot soldiers in this sprawling system, with their indoctrination beginning in the academic institutions that are subsidized by the very same cartel. They have turned into executors of institutions, no longer focusing on patient welfare but merely acting as drug couriers for the pharmaceutical cartel.
In contrast, doctors receive very little training in nutrition. Physicians and pediatricians have been indoctrinated into the medical industry, no longer serving as independent healers but as mere “brokers” and “salespeople” for pharmaceutical companies.
Doctors prescribe antibiotics that destroy beneficial bacteria, reducing the body's ability to digest and assimilate food and hinder its innate Vital Force. They prescribe 13 or more pills a day to patients, diagnose conditions like ADHD because it's easy, and prescribe dangerous and addictive medications rather than simply advising their patients to eat in an alignment to their core essence.
"Consult your physician!"—a phrase we hear constantly all around and from deceptive advertisements on television is ingrained in everyone's mind. Today, advising someone to brew herbal tea is met with bone-shaking fear due to the cartel's fear-mongering propaganda, which has established full control within the spirit of humanity.

The irony is that despite the financial support, public trust, and large-scale testing and trials of all their methods and theories, medical schools have completely failed to control any of the deadly diseases and have not found a safe cure for even one mild illness. Modern medicine attempts to protect humans from rapidly fatal infections but leaves them vulnerable to slower, more brutal diseases.
As our species progressed industrially and technologically, it seems we traded a high rate of deadly infectious diseases for a growing epidemic of chronic, neurological and autoimmune conditions, along with a steady rise in all forms of cancer. As far as I can tell, this trend started about 150-200 years ago. Never in human history have preventable diseases thrived so much, continuously fueled by the very drugs and irritants that commercialized them in the first place.
We cannot criticize someone for using drugs, until we, ourselves, cease the usage of medications, or alternatively, keep using medications and cease to judge others for using drugs. We can't eat the cake and have it.
The more we keep absconding from confronting the hypocritical behavior within ourselves, we’ll never be able to see the eradication of the drug-culture, as well as the pharmaceutical complex.
For in truth, they're one and the same.